Atrial Fibrillation
| This is part of: Supraventricular Rhythms |
| {{{locatieafbeelding}}} | |
| Atrial rate | 400-600 bpm |
| Ventricular rate | 75-175 bpm |
| Regularity | irregular |
| Origin | atria (SVT) |
| P-wave | absent |
| Effect of adenosine | reduces heart rate |
| Example ECG: {{{example}}} | |
| Example ECG2: {{{example2}}} | |
During atrial fibrillation the atria show chaotic depolarisation with multiple foci. Mechanically the atria stop contracting after several days to weeks of atrial fibrillation, the result of the ultra-rapid depolarisations that occur in the atria, typically around 400 bpm, but up to 600 bpm. At the AV node 'every now and then' a beat is conducted to the ventricles, resulting in an irregular ventricular rate, which is the typical ECG characteristic of atrial fibrillation. Sometimes atrial fibrillation results in a course atrial flutter wave on the ECG, but the baseline can also be flat. A flat baseline is more often seen in long standing atrial fibrillation. The cardiac stroke volume is reduced by 10-20% during atrial fibrillation, as the 'atrial kick' is missing and because the heart does not have time to fill at the often higher ventricular rate. Causes age (+- 10% of 70+ year olds and 15% of 90+ year olds have AFIB kelley), ischemia, hyperthyreoidism, alcohol abuse.
Atrial fibrillation can be catechorized as follows:
- First documented episode
- Recurrent atrial fibrillation: after two or more episodes.
- Paroxysmal atrial fibrillation: if recurrent atrial fibrillation spontaneously converts to sinus rhythm.
- Persisting atrial fibrillation: if an episode of atrial fibrillation persists more than 7 days.
- Permanent atrial fibrillation: if atrial fibrillation persists after an effort of electrical or chemical cardioversion
Lone AF is atrial fibrillation in patients younger than 60 years in whom no clinical or electrocardiographic signs of heart or lung disease are present. These patiens have a favourable prognosis regarding thrombo-embolic events.
Non-valvular atrial fibrillation is atrial fibrillation in patients without heart valve disease or heart valve replacement or repair. ESCAF
Treatment strategies include:RACEPIAFSTAF
- Rate control: accept atrial fibrillation and focus on symptom relief and prevention of tachycardias. Typically with beta-blockers and digoxin. Target rate is < 100 bpm.
- Rhythm control: trying to keep the patient in normal sinus rhythm. Typically with anti-arrhythmics like amiodarone, flecainide, and sotalol, or electrical cardioversion, or with radiofrequency catheter ablation.
In both cases anti-coagulants are needed to prevent embolic stroke.
Examples
-
 Atrial fibrillation with reasonable rate control
Atrial fibrillation with reasonable rate control -
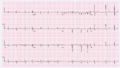
 Atrial fibrillation with rapid ventricular rate
Atrial fibrillation with rapid ventricular rate -
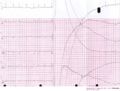
 Detail of atrial fibrillation with rapid ventricular rate
Detail of atrial fibrillation with rapid ventricular rate -
 Atrial fibrillation electrically cardioverted into sinusrhythm
Atrial fibrillation electrically cardioverted into sinusrhythm -
 atrial fibrillation with marked organization in V1 (which is close to the right atrial appendage), this is not atrial flutter.
atrial fibrillation with marked organization in V1 (which is close to the right atrial appendage), this is not atrial flutter.




References
<biblio>
- ESCAF pmid=16885201
- kelley pmid=17126661
- RACE pmid=12466507
- PIAF pmid=11117910
- STAF pmid=12767648
</biblio>