Approach to the Wide Complex Tachycardia: Difference between revisions
Jump to navigation
Jump to search
mNo edit summary |
|||
| Line 1: | Line 1: | ||
During wide complex tachycardia (heart rate > 100/min, QRS > 0.12 sec) the differentiation between supraventricular and ventricular origin of the arrhythmia is important to guide therapy. Several algorhythms have been developed to aid in this differentiation. | |||
== The ACC algorhythm <cite>ACC</cite>== | == The ACC algorhythm <cite>ACC</cite>== | ||
[[File:VT_algorythm_en.png|800px|thumb|left|SVT vs VT algorhytm. Adapted from <cite>ACC</cite>]] | [[File:VT_algorythm_en.png|800px|thumb|left|SVT vs VT algorhytm. Adapted from <cite>ACC</cite>]] | ||
{{clr}} | {{clr}} | ||
== Brugada criteria | == Brugada criteria == | ||
{| class="wikitable" width="500px" | {| class="wikitable" width="500px" | ||
! colspan="3" |Brugada criteria ter differentiatie van [[supraventriculaire ritmestoornissen]] (SVT's) van [[ventriculaire ritmestoornissen]] (VT's)<cite>Brug1</cite> | ! colspan="3" |Brugada criteria ter differentiatie van [[supraventriculaire ritmestoornissen]] (SVT's) van [[ventriculaire ritmestoornissen]] (VT's)<cite>Brug1</cite> | ||
Revision as of 11:09, 11 November 2009
During wide complex tachycardia (heart rate > 100/min, QRS > 0.12 sec) the differentiation between supraventricular and ventricular origin of the arrhythmia is important to guide therapy. Several algorhythms have been developed to aid in this differentiation.
The ACC algorhythm ACC

Brugada criteria
| Brugada criteria ter differentiatie van supraventriculaire ritmestoornissen (SVT's) van ventriculaire ritmestoornissen (VT's)Brug1 | ||
|---|---|---|
| Zijn er fusie of capture beats? (dit item komt niet uit de Brugada criteria, maar is wel heel specifiek) | Ja? => VT | specificiteit=100%  |
| RS complexen afwezig over de voorwand? | Ja? => VT | sensitiviteit=21% specifiteit=100% |
| RS-interval in één van de precordiale afleidingen > 100 msec (bij patient zonder anti-arritmetica)? | Ja? => VT | sensitiviteit=66% specifiteit=98% |
| Is er AV-dissociatie? | Ja? => waarschijnlijk VT (NB AV nodale re-entry kan ook AV-dissociatie geven!) | sensitiviteit=82% specifiteit=98% |
| Morfologische criteria (als bovenstaande criteria geen uitkomst bieden) | ||
| LBTB patroon | ||
| Initiële R breder dan 40ms? | Ja => VT | thumb|100px |
| Slurred of notched neergaand been van S golf in afleiding V1 of V2 | Ja => VT | |
| Begin Q tot nadir QS >60 ms in V1 of V2? | Ja => VT | LR >50:1 |
| Q of QS in V6? | Ja => VT | LR >50:1 |
| thumb|300px | ||
| RBTB patroon | ||
| Monofasische R of qR in V1? | Ja => VT | |
| R hoger dan R' (rabbit-ear sign)? | Ja => VT | LR >50:1 |
| rS in V6? | Ja => VT | LR >50:1 |
| thumb|300px | ||
Voorbeelden
-
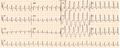 Breedcomplextachycardie. Geen AV dissociatie. RBTB. Lijkt op complex bij SR van zelfde patient. Conclusie: SVT met aberrantie
Breedcomplextachycardie. Geen AV dissociatie. RBTB. Lijkt op complex bij SR van zelfde patient. Conclusie: SVT met aberrantie -
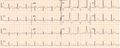 ECG van zelfde patient als eerste voorbeeld, maar nu in sinusritme. Het QRS complex is nauwelijks gewijzigd
ECG van zelfde patient als eerste voorbeeld, maar nu in sinusritme. Het QRS complex is nauwelijks gewijzigd -
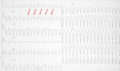 Breedcomplextachycardie. LBTB configuratie. Afwezigheid RS over voorwand. AV-dissociatie: de pijlen wijzen de p-toppen aan. Conclusie: ventrikeltachycardie
Breedcomplextachycardie. LBTB configuratie. Afwezigheid RS over voorwand. AV-dissociatie: de pijlen wijzen de p-toppen aan. Conclusie: ventrikeltachycardie -
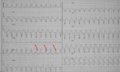 Breedcomplextachycardie. LBTB configuratie. Afwezigheid RS over vorwand. AV-dissociatie: de pijlen wijzen de p-toppen aan. Conclusie: ventrikeltachycardie
Breedcomplextachycardie. LBTB configuratie. Afwezigheid RS over vorwand. AV-dissociatie: de pijlen wijzen de p-toppen aan. Conclusie: ventrikeltachycardie


{kind=link}
{kind=link}
{kind=link}
Referenties
<biblio>
- ACC pmid=14563598
- Brug1 pmid=2022022
</biblio>