Introduction to Arrhythmias: Difference between revisions
Jump to navigation
Jump to search
No edit summary |
No edit summary |
||
| Line 22: | Line 22: | ||
* What is the '''[[Conduction|QRS width]]'''? | * What is the '''[[Conduction|QRS width]]'''? | ||
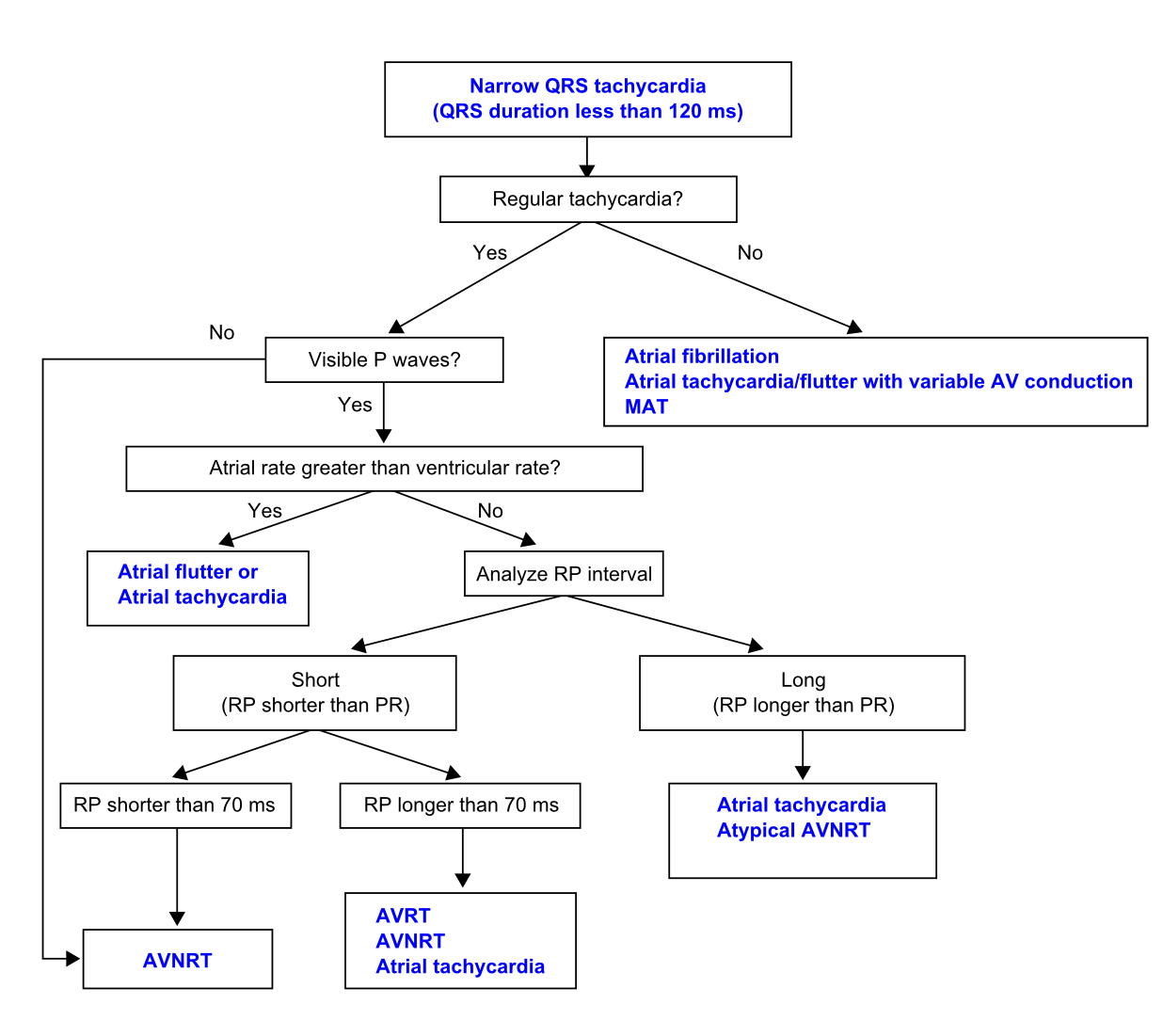
**If the QRS < 120ms (i.e. a narrow complex), then it is either a [[Sinus node rhythms and arrhythmias|sinus arrhythmia]], [[Supraventricular Rhythms|supraventricular rhythm]] or a [[Junctional Tachycardias|junctional tachycardia]]. In tachycardias, this [[Media:Svt_algorythm_en.png|'''flowchart''']] will lead to the right diagnosis.<cite>ESCnarrowQRS</cite> | **If the QRS < 120ms (i.e. a narrow complex), then it is either a [[Sinus node rhythms and arrhythmias|sinus arrhythmia]], [[Supraventricular Rhythms|supraventricular rhythm]] or a [[Junctional Tachycardias|junctional tachycardia]]. In tachycardias, this [[Media:Svt_algorythm_en.png|'''flowchart''']] will lead to the right diagnosis.<cite>ESCnarrowQRS</cite> | ||
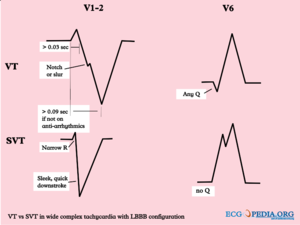
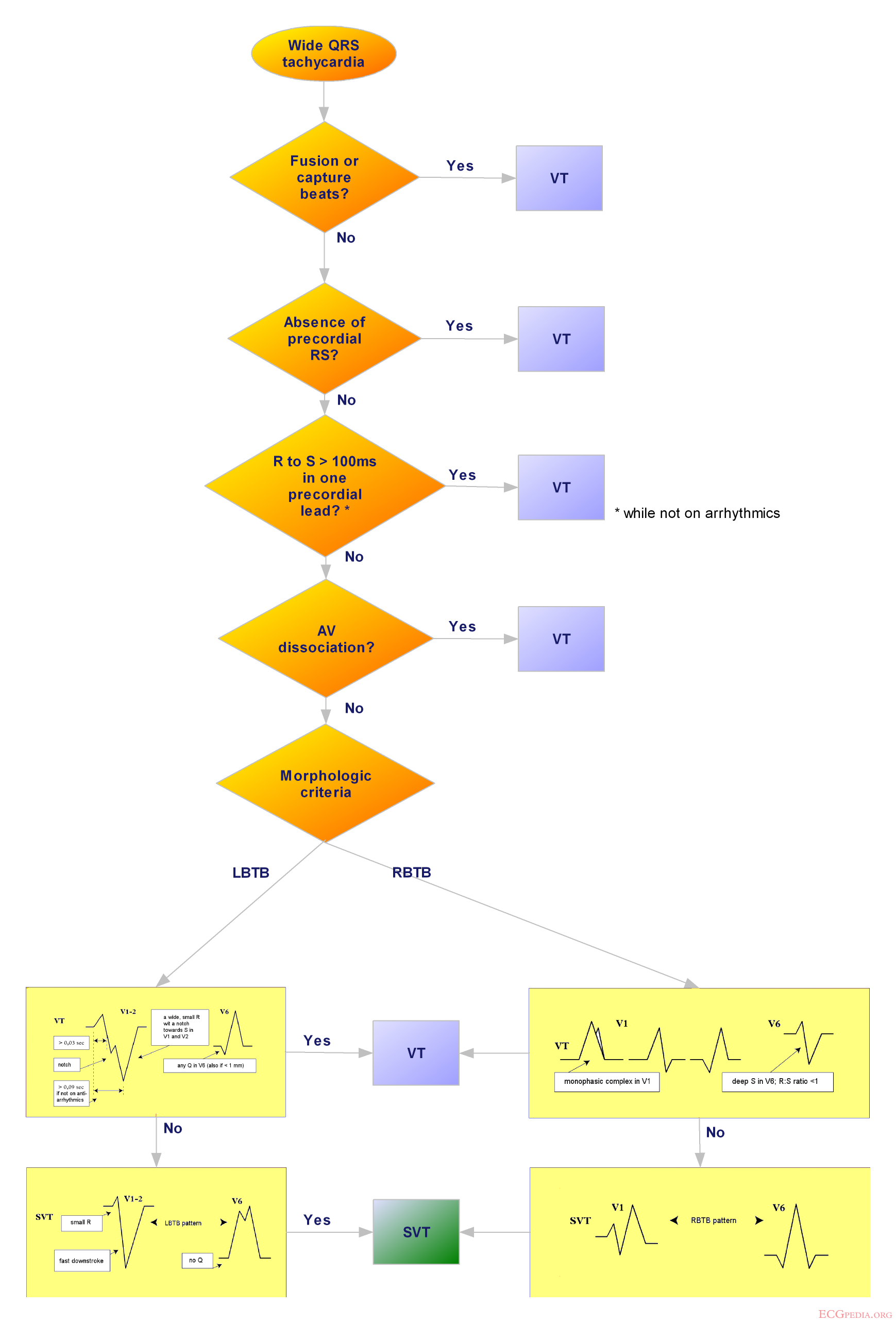
**If the QRS > 120ms it is either a [[Ventricular Arrhythmias|ventricular tachycardia]] or a [[Supraventricular Rhythms|supraventricular rhythm]] with additional [[Intraventricular Conduction|bundle branch block]]. This is a challenging | **If the QRS > 120ms it is either a [[Ventricular Arrhythmias|ventricular tachycardia]] or a [[Supraventricular Rhythms|supraventricular rhythm]] with additional [[Intraventricular Conduction|bundle branch block]]. This is a challenging diagnosis. Therefore a [[media:wideQRS_tachycardia_flow.png|'''flowchart''']] which incoporates the Brugada criteria for VT should be used.<cite>Brugada</cite> Another method to discriminate VT from SVT has been proposed by Vereckei et al.<cite>vereckei</cite>In that paper an excellent review is given on the subject by Dendi and Josephson.<cite>dendi</cite> | ||
* What is the '''[[Heart axis|Heart Axis]]''' and did it change? | * What is the '''[[Heart axis|Heart Axis]]''' and did it change? | ||
** If the heart axis turns significantly when compared to the heart axis during sinus rhythm a ventricular origin of the rhythm is more likely. | ** If the heart axis turns significantly when compared to the heart axis during sinus rhythm a ventricular origin of the rhythm is more likely. | ||
Revision as of 19:55, 27 January 2010
| Author(s) | J.S.S.G. de Jong | |
| Moderator | J.S.S.G. de jong | |
| Supervisor | ||
| some notes about authorship | ||

Morphologic criteria to differentiate between SVT vs. VT in a wide complex tachycardia. This is part of the wide complex tachycardia flowchart
{kind=link}
Arrhythmias (non-normal heart rhythms) can be a challenge to understand, but with a systematic approach, diagnosis is often less difficult than it may appear at first.
A good stepwise approach to interpret the heart rhythm is to follow these steps:
- What is the ventricular heart rate?
- >100 bpm = tachycardia
- <60 bpm = bradycardia
- are there extra beats? -> Ectopic Beats
- Cherchez le P, French for find the P waves.
- Do you see P waves? Leads II and V1 are often most suitable to find P waves.
- What is the rate of the P waves?
- What is the P wave morphology?
- What is the relationship between P waves and QRS complexes?
- Is there a 1:1 relation between P waves and QRS complexes? If not there may be AV dissociation due to a Ventricular Arrhythmias or AV block
- Is every P wave followed by a QRS complex? And every QRS preceded by a P wave?
- What is the PR interval and does it change?
- What is the QRS width?
- If the QRS < 120ms (i.e. a narrow complex), then it is either a sinus arrhythmia, supraventricular rhythm or a junctional tachycardia. In tachycardias, this flowchart will lead to the right diagnosis.[1]
- If the QRS > 120ms it is either a ventricular tachycardia or a supraventricular rhythm with additional bundle branch block. This is a challenging diagnosis. Therefore a flowchart which incoporates the Brugada criteria for VT should be used.[2] Another method to discriminate VT from SVT has been proposed by Vereckei et al.[3]In that paper an excellent review is given on the subject by Dendi and Josephson.[4]
- What is the Heart Axis and did it change?
- If the heart axis turns significantly when compared to the heart axis during sinus rhythm a ventricular origin of the rhythm is more likely.
- What is the clinical setting?
- A wide complex tachycardia in a hemodynamically unstable 70-year-old man with previous myocardial infarction should be considered a ventricular tachycardia until proven otherwise
- A wide complex tachycardia in a 24-year-old woman with recurrent spells of tachycardia that respond to vagal maneuvers is most likely an AVNRT with aberrant conduction.
{kind=link}
References
- Blomström-Lundqvist C, Scheinman MM, Aliot EM, Alpert JS, Calkins H, Camm AJ, Campbell WB, Haines DE, Kuck KH, Lerman BB, Miller DD, Shaeffer CW, Stevenson WG, Tomaselli GF, Antman EM, Smith SC Jr, Alpert JS, Faxon DP, Fuster V, Gibbons RJ, Gregoratos G, Hiratzka LF, Hunt SA, Jacobs AK, Russell RO Jr, Priori SG, Blanc JJ, Budaj A, Burgos EF, Cowie M, Deckers JW, Garcia MA, Klein WW, Lekakis J, Lindahl B, Mazzotta G, Morais JC, Oto A, Smiseth O, Trappe HJ, and European Society of Cardiology Committee, NASPE-Heart Rhythm Society. ACC/AHA/ESC guidelines for the management of patients with supraventricular arrhythmias--executive summary. a report of the American college of cardiology/American heart association task force on practice guidelines and the European society of cardiology committee for practice guidelines (writing committee to develop guidelines for the management of patients with supraventricular arrhythmias) developed in collaboration with NASPE-Heart Rhythm Society. J Am Coll Cardiol. 2003 Oct 15;42(8):1493-531. DOI:10.1016/j.jacc.2003.08.013 |
- Brugada P, Brugada J, Mont L, Smeets J, and Andries EW. A new approach to the differential diagnosis of a regular tachycardia with a wide QRS complex. Circulation. 1991 May;83(5):1649-59. DOI:10.1161/01.cir.83.5.1649 |
- Vereckei A, Duray G, Szénási G, Altemose GT, and Miller JM. Application of a new algorithm in the differential diagnosis of wide QRS complex tachycardia. Eur Heart J. 2007 Mar;28(5):589-600. DOI:10.1093/eurheartj/ehl473 |
- Dendi R and Josephson ME. A new algorithm in the differential diagnosis of wide complex tachycardia. Eur Heart J. 2007 Mar;28(5):525-6. DOI:10.1093/eurheartj/ehl557 |