McGill Case 86: Difference between revisions
Jump to navigation
Jump to search
(Created page with "{{McGillcase| |previouspage= McGill Case 85 |previousname= McGill Case 85 |nextpage= McGill Case 87 |nextname= McGill Case 87 }} [[File:E000786.jpg|thumb|600px|left|This rhyt...") |
No edit summary |
||
| (One intermediate revision by the same user not shown) | |||
| Line 6: | Line 6: | ||
}} | }} | ||
[[File: | [[File:E000788.jpg|thumb|600px|left|Comment | ||
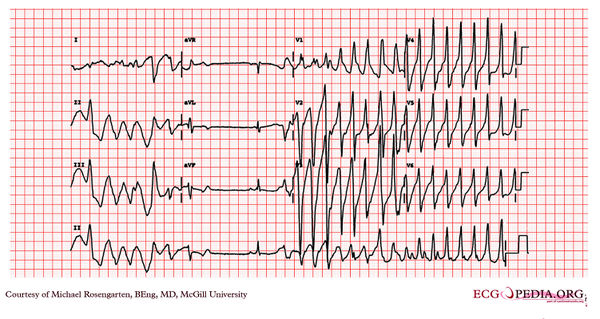
This is a classic 12 lead EKG of a patient with Torsade de Pointes. | |||
It shows the polymorphic nature of the tachycardia, the long QT interval and the initiation of the tachycardia with a late coupled P.V.C. | |||
Torsade is a polymorphic tachycaridia that is associated with prolongation of the QT interval (usually greater than 600 ms) and can be acquired or congenital. This arrhythmia was responsible for Quinidine syncope and is an important cause of sudden death in patients treated with type I and type III antiarrhythmic medications. The electrical mechanism may be related to dispersion of repolarization or to triggered activity associated with after depolarizations. | |||
Besides medications, acquired Torsade can be associated with hypokalemia, and a slow heart rate (complete heart block). This patient was a renal patient on dialysis who was admitted to hospital for an E.N.T. operation on one of her sinuses. The arrhythmia was noted during the operation. At the time of the procedure she was taking sotalol and this combined with her renal failure was the presumed cause of the arrhythmia. | |||
Sotalol has both class II (beta-blocking) and class III (prolonging of action potential) effects. Sotalol is excreted mainly by the kidneys and the dosing intervals should be lengthened when the creatinine clearance is less than 60 ml/min. As with the anti-arrhythmic effect of sotalol, Torsade de pointes is dose dependent and occurs in 0.5 percent of patients who taking 160 mg/day, 1.6 % taking 320 mg/day, and up to 5.8% taking more than 320 mg/day. | |||
The arrhythmia in this patient did not recurred post-operatively with the sotalol removed from her medications. | |||
]] | |||
Latest revision as of 04:46, 15 February 2012
|

Comment This is a classic 12 lead EKG of a patient with Torsade de Pointes. It shows the polymorphic nature of the tachycardia, the long QT interval and the initiation of the tachycardia with a late coupled P.V.C. Torsade is a polymorphic tachycaridia that is associated with prolongation of the QT interval (usually greater than 600 ms) and can be acquired or congenital. This arrhythmia was responsible for Quinidine syncope and is an important cause of sudden death in patients treated with type I and type III antiarrhythmic medications. The electrical mechanism may be related to dispersion of repolarization or to triggered activity associated with after depolarizations. Besides medications, acquired Torsade can be associated with hypokalemia, and a slow heart rate (complete heart block). This patient was a renal patient on dialysis who was admitted to hospital for an E.N.T. operation on one of her sinuses. The arrhythmia was noted during the operation. At the time of the procedure she was taking sotalol and this combined with her renal failure was the presumed cause of the arrhythmia. Sotalol has both class II (beta-blocking) and class III (prolonging of action potential) effects. Sotalol is excreted mainly by the kidneys and the dosing intervals should be lengthened when the creatinine clearance is less than 60 ml/min. As with the anti-arrhythmic effect of sotalol, Torsade de pointes is dose dependent and occurs in 0.5 percent of patients who taking 160 mg/day, 1.6 % taking 320 mg/day, and up to 5.8% taking more than 320 mg/day. The arrhythmia in this patient did not recurred post-operatively with the sotalol removed from her medications.