McGill Case 263: Difference between revisions
Jump to navigation
Jump to search
(Created page with "{{McGillcase| |previouspage= McGill Case 262 |previousname= McGill Case 262 |nextpage= McGill Case 264 |nextname= McGill Case 264 }} [[File:E263.jpg|thumb|600px|left|This is ...") |
No edit summary |
||
| Line 6: | Line 6: | ||
}} | }} | ||
[[File:E263.jpg|thumb|600px|left|This is | [[File:E263.jpg|thumb|600px|left|This is a recording from a patient being treated for a wide complex tachycardia . The recording could be sinus with a first degree block (plus a partial right bundle branch block or possibly RVH). It is to be noted though that a sinus rate of 100/min seems some what fast for a patient on nadolol and that the rhythm is irregular. | ||
On the other hand, the more likely rhyhtm is SVT (or slow atrial flutter at a rate of 200/min) with variable block though mostly 2:1 block. This is an atrial rate similar to that of the wide complex tachycardia, and if one looks in lead I and lead V1 there does appear to be atrial activity at twice the ventricular rate. | |||
]] | |||
Latest revision as of 21:05, 19 February 2012
|

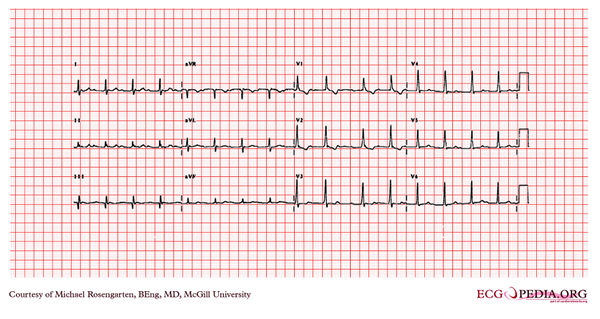
This is a recording from a patient being treated for a wide complex tachycardia . The recording could be sinus with a first degree block (plus a partial right bundle branch block or possibly RVH). It is to be noted though that a sinus rate of 100/min seems some what fast for a patient on nadolol and that the rhythm is irregular. On the other hand, the more likely rhyhtm is SVT (or slow atrial flutter at a rate of 200/min) with variable block though mostly 2:1 block. This is an atrial rate similar to that of the wide complex tachycardia, and if one looks in lead I and lead V1 there does appear to be atrial activity at twice the ventricular rate.