MI Diagnosis in LBBB or paced rhythm

In case of a left bundle branch block (LBBB), infarct diagnosis based on the ECG is difficult. The baseline ST segments and T waves tend to be shifted in a discordant direction with LBBB, which can mask or mimic acute myocardial infarction. However, serial ECGs may show a moving ST segment during ischemia secondary to dynamic supply versus demand characteristics. A new LBBB is always pathological and can be a sign of myocardial infarction. The criteria (Sgarbossa [1]) that can be used in case of a LBBB and suspicion of infarction are:
- ST elevation > 1mm in leads with a positive QRS complex (concordance in ST deviation) (score 5)
- ST depression > 1 mm in V1-V3 (concordance in ST deviation) (score 3)
- ST elevation > 5 mm in leads with a negative QRS complex (inappropriate discordance in ST deviation) (score 2). This criterion is sensitive, but not specific for ischemia in LBBB. It is however associated with a worse prognosis, when present in LBBB during ischemia.[2]
At a score-sum of 3, these criteria have a specificity of 90% for detecting a myocardial infarction.
During right ventricular pacing the ECG also shows left bundle brach block and the above rules also apply for the diagnosis of myocardial infarction during pacing, however they are less specific.[3][4] In the GUSTO-1 trial the ECG criterion with a high specificity and statistical significance for the diagnosis of an acute MI was:[5]
- ST segment elevation ≥5 mm in leads with a negative QRS complex.
Two other criteria with acceptable specificity were:
- ST elevation ≥1 mm in leads with concordant QRS polarity
- ST depression ≥1 mm in leads V1, V2, or, V3
Examples

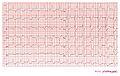
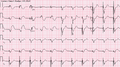
Case 1: Acute myocardial infarction in in a patient with a pacemaker and LBBB. Concordant ST elevation in V5-V6 are clearly visible. There is discordant ST segment elevation > 5 mm in lead V3.

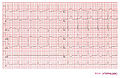
Case 1: The same patient as in the first example 2 months before the myocardial infarction. Normal LBBB pattern.
Case 2: Acute MI in a patient with LBBB
Case 3: Acute MI in a patient with LBBB
Case 3: Non-ischemic ECG in this patient

Myocardial infarction in a pacemaker patient. The ECG shows LBBB as expected during pacing, however overt repolarization abnormalities are present.
Myocardial infarction post primary PCI in a pacemaker patient
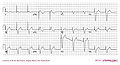
Ventricular pacemaker with acute inferior infarction







References
- Sgarbossa EB, Pinski SL, Barbagelata A, Underwood DA, Gates KB, Topol EJ, Califf RM, and Wagner GS. Electrocardiographic diagnosis of evolving acute myocardial infarction in the presence of left bundle-branch block. GUSTO-1 (Global Utilization of Streptokinase and Tissue Plasminogen Activator for Occluded Coronary Arteries) Investigators. N Engl J Med. 1996 Feb 22;334(8):481-7. DOI:10.1056/NEJM199602223340801 |
- Wong CK, French JK, Aylward PE, Stewart RA, Gao W, Armstrong PW, Van De Werf FJ, Simes RJ, Raffel OC, Granger CB, Califf RM, White HD, and HERO-2 Trial Investigators. Patients with prolonged ischemic chest pain and presumed-new left bundle branch block have heterogeneous outcomes depending on the presence of ST-segment changes. J Am Coll Cardiol. 2005 Jul 5;46(1):29-38. DOI:10.1016/j.jacc.2005.02.084 |
- Klimczak A, Wranicz JK, Cygankiewicz I, Chudzik M, Goch JH, and Baranowski R. Electrocardiographic diagnosis of acute coronary syndromes in patients with left bundle branch block or paced rhythm. Cardiol J. 2007;14(2):207-13.
- Madias JE. The nonspecificity of ST-segment elevation > or =5.0 mm in V1-V3 in the diagnosis of acute myocardial infarction in the presence of ventricular paced rhythm. J Electrocardiol. 2004 Apr;37(2):135-9. DOI:10.1016/j.jelectrocard.2004.01.008 |
- Sgarbossa EB, Pinski SL, Gates KB, and Wagner GS. Early electrocardiographic diagnosis of acute myocardial infarction in the presence of ventricular paced rhythm. GUSTO-I investigators. Am J Cardiol. 1996 Feb 15;77(5):423-4. DOI:10.1016/s0002-9149(97)89377-0 |