Ventricular pre-excitation (Wolff-Parkinson-White pattern): Difference between revisions
No edit summary |
mNo edit summary |
||
| (14 intermediate revisions by 6 users not shown) | |||
| Line 1: | Line 1: | ||
[[Image:wolffparkinsonwhite.jpg|thumb| Louis Wolff, Sir John Parkinson and Paul Dudley, who discovered the phenomenon that later would be called the WPW syndrome.]] | [[Image:wolffparkinsonwhite.jpg|thumb| Louis Wolff, Sir John Parkinson and Paul Dudley White, who discovered the phenomenon that later would be called the WPW syndrome.]] | ||
[[Image:Rhythm_WPW.png|thumb| The upstroke of the QRS-complex is 'slurred', resulting in a delta-wave (arrow).]] | [[Image:Rhythm_WPW.png|thumb| The upstroke of the QRS-complex is 'slurred', resulting in a delta-wave (arrow).]] | ||
[[Image: | [[Image:wpw2.svg|thumb|Conduction through the accessory pathway results in a delta wave.]] | ||
[[Image:OCT_ACT.svg|thumb| A atrioventricular tachycardia through the accessory bundle. The electrical signal travels from the ventricles via the accessory bundle to the atria and returns to the ventricles via the AV node.]] | |||
In 1930 Louis Wolff, Sir John Parkinson and Paul Dudley White described 11 patients who suffered from bouts of tachcyardias. Their ECGs showed two abnormalities: a short PQ time and a delta-wave. | In 1930 Louis Wolff, Sir John Parkinson and Paul Dudley White described 11 patients who suffered from bouts of tachcyardias. Their ECGs showed two abnormalities: a short PQ time and a delta-wave. | ||
Ever since one speaks of the '''Wolff-Parkinson-White syndrome''' in patients with complaints of syncope and / or tachycardia and a pre-exitation pattern on the ECG (WPW syndrome = WPW pattern + symptoms). Not all patients with a WPW ''pattern'' on the ECG are symptomatic. The prevalence of the WPW or pre-exitation pattern is relatively common in the general population about 0.15-0.25%. | Ever since one speaks of the '''Wolff-Parkinson-White syndrome''' in patients with complaints of syncope and / or tachycardia and a pre-exitation pattern on the ECG (WPW syndrome = WPW pattern + symptoms). Not all patients with a WPW ''pattern'' on the ECG are symptomatic. The prevalence of the WPW or pre-exitation pattern is relatively common in the general population (about 0.15-0.25%). | ||
The pre-exitation pattern is caused by an extra connection between the atria and the ventricles (accessory bundle) that forms an electrical bypass to the AV node. The part of the ventricle where this accessory bundle connects are the first to depolarize. This is shown on the ECG as a delta wave. The QRS-complex is somewhat widened (> 0.10 sec). Also the PQ time is shorter (< 0.12 sec). By observing the pattern of the delta wave in the different leads, one can estimate the location of the accessory bundle. | The pre-exitation pattern is caused by an extra connection between the atria and the ventricles (accessory bundle) that forms an electrical bypass to the AV node. The part of the ventricle where this accessory bundle connects are the first to depolarize. This is shown on the ECG as a delta wave. The QRS-complex is somewhat widened (> 0.10 sec). Also the PQ time is shorter (< 0.12 sec). By observing the pattern of the delta wave in the different leads, one can estimate the location of the accessory bundle. | ||
| Line 26: | Line 26: | ||
WPW can be treated by destroying the accessory bundle with ablation therapy.<cite>Pappone</cite> Depending on the type of arrhythmias that occur anti-arrhythmic therapy can play a role. | WPW can be treated by destroying the accessory bundle with ablation therapy.<cite>Pappone</cite> Depending on the type of arrhythmias that occur anti-arrhythmic therapy can play a role. | ||
{{clr}} | {{clr}} | ||
== Determining the location of the accessory pathway == | |||
By closely observing the shape of the delta wave on the ECG, the location of the accessory connection can often be estimated. Several algorithms have been developed for this purpose.<cite>Milstein</cite> | |||
[[Image:Pathway_nomenclature.png|thumb|left|300px|Seen from the apex, the tricuspid and mitral valve form a plane, relative to which the accessory connections are named.<cite>cosio</cite>]] | |||
[[Image:Pathway_prevalence.png|thumb|right|300px|Large differences in prevalence of accessory bundle location]] | |||
[[Image:Milstein_algorythm.png|thumb|300px|The Milstein algorhythm is relatively straightforward. Adapted from: <cite>Milstein</cite>]] | |||
[[Image:Arruda_algorhythm.png|thumb|left|300px|The Arruda algorhythm. Adapted from: <cite>Arruda</cite>]] | |||
{{clr}} | |||
== Examples == | |||
<gallery> | |||
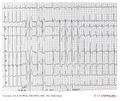
Image:wpw_full_ecg.jpg|WPW on a 12 lead ECG | |||
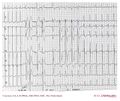
Image:wpw_full_ecg2.jpg|Another example of pre-exitation on a 12 lead ECG | |||
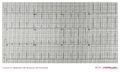
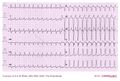
Image:wpw_full_ecg3.png|Another example of WPW on a 12 lead ECG | |||
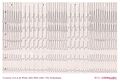
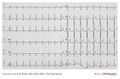
Image:ECG000029.jpg| Atrial fibrillation in a patient with WPW: Fast Broad Irregular (FBI) | |||
Image:ECG000030.jpg| Same patient as above during sinus rhythm: evident delta wave | |||
Image:AW00001.png | |||
Image:AW00002.png | |||
Image:AW00003.jpg | |||
Image:AW00004.jpg | |||
Image:AW0005.jpg | |||
Image:AW0006.jpg | |||
Image:AW0007.jpg | |||
Image:AW0008.jpg | |||
Image:AW0009.jpg | |||
Image:AW00010.jpg | |||
Image:AW00011.jpg | |||
Image:AW00012.jpg | |||
Image:AW00013.jpg | |||
Image:AW00014.jpg | |||
</gallery> | |||
== References == | == References == | ||
<biblio> | <biblio> | ||
#cosio pmid=10413636 | |||
#Pappone pmid=14602878 | #Pappone pmid=14602878 | ||
#Milstein pmid=2440006 | |||
#Arruda pmid=9475572 | |||
</biblio> | </biblio> | ||
Latest revision as of 17:15, 18 December 2012




In 1930 Louis Wolff, Sir John Parkinson and Paul Dudley White described 11 patients who suffered from bouts of tachcyardias. Their ECGs showed two abnormalities: a short PQ time and a delta-wave.
Ever since one speaks of the Wolff-Parkinson-White syndrome in patients with complaints of syncope and / or tachycardia and a pre-exitation pattern on the ECG (WPW syndrome = WPW pattern + symptoms). Not all patients with a WPW pattern on the ECG are symptomatic. The prevalence of the WPW or pre-exitation pattern is relatively common in the general population (about 0.15-0.25%).
The pre-exitation pattern is caused by an extra connection between the atria and the ventricles (accessory bundle) that forms an electrical bypass to the AV node. The part of the ventricle where this accessory bundle connects are the first to depolarize. This is shown on the ECG as a delta wave. The QRS-complex is somewhat widened (> 0.10 sec). Also the PQ time is shorter (< 0.12 sec). By observing the pattern of the delta wave in the different leads, one can estimate the location of the accessory bundle.
The risk of having an accessory bundle is the development of tachycardias. Two forms of tachycardias exist:
- An atrioventricular tachcyardia, in which the electrical signal from the ventricles is conducted back to the atria. These fast arrhythmias (> 200 bpm) can deteriorate into ventricular fibrillation and sudden death.
- A supraventricular tachycardia with 1:1 conduction through the accessory bundle. A typical example is atrial fibrillation. Atrial fibrillation in WPW can result in a fast and irregular tachycardia: Fast, Broad & Irregular (FBI). This fast arrhythmia also carries the risk to deteriorate into ventricular fibrillation and sudden death.
In clinical practice it is therefore important to distinguish benign from malign accessory bundles.
Characteristics of a benign accessory bundle
- Intermittant WPW pattern on Holter registration
- Sudden disappearing of the pre-exitation pattern during exercise testing.
- The accessory bundle responds to blockade by medication (especially sodium channel blockers)
Characteristics of a malign accessory bundle
- The occurence of very fast arrhythmias during spontanous attacks of atrial fibrillation (> 240 bpm).
WPW can be treated by destroying the accessory bundle with ablation therapy.[1] Depending on the type of arrhythmias that occur anti-arrhythmic therapy can play a role.
Determining the location of the accessory pathway
By closely observing the shape of the delta wave on the ECG, the location of the accessory connection can often be estimated. Several algorithms have been developed for this purpose.[2]




Examples
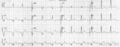
WPW on a 12 lead ECG
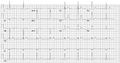
Another example of pre-exitation on a 12 lead ECG

Another example of WPW on a 12 lead ECG

Atrial fibrillation in a patient with WPW: Fast Broad Irregular (FBI)
Same patient as above during sinus rhythm: evident delta wave



























References
- Pappone C, Santinelli V, Manguso F, Augello G, Santinelli O, Vicedomini G, Gulletta S, Mazzone P, Tortoriello V, Pappone A, Dicandia C, and Rosanio S. A randomized study of prophylactic catheter ablation in asymptomatic patients with the Wolff-Parkinson-White syndrome. N Engl J Med. 2003 Nov 6;349(19):1803-11. DOI:10.1056/NEJMoa035345 |
- Milstein S, Sharma AD, Guiraudon GM, and Klein GJ. An algorithm for the electrocardiographic localization of accessory pathways in the Wolff-Parkinson-White syndrome. Pacing Clin Electrophysiol. 1987 May;10(3 Pt 1):555-63. DOI:10.1111/j.1540-8159.1987.tb04520.x |
- Cosío FG, Anderson RH, Becker A, Borggrefe M, Campbell RW, Gaita F, Guiraudon GM, Haïssaguerre M, Kuck KJ, Rufilanchas JJ, Thiene G, Wellens HJ, Langberg J, Benditt DG, Bharati S, Klein G, Marchlinski F, and Saksena S. Living anatomy of the atrioventricular junctions. A guide to electrophysiological mapping. A Consensus Statement from the Cardiac Nomenclature Study Group, Working Group of Arrythmias, European Society of Cardiology, and the Task Force on Cardiac Nomenclature from NASPE. North American Society of Pacing and Electrophysiology. Eur Heart J. 1999 Aug;20(15):1068-75. DOI:10.1053/euhj.1999.1657 |
- Arruda MS, McClelland JH, Wang X, Beckman KJ, Widman LE, Gonzalez MD, Nakagawa H, Lazzara R, and Jackman WM. Development and validation of an ECG algorithm for identifying accessory pathway ablation site in Wolff-Parkinson-White syndrome. J Cardiovasc Electrophysiol. 1998 Jan;9(1):2-12. DOI:10.1111/j.1540-8167.1998.tb00861.x |