Test: Difference between revisions
Jump to navigation
Jump to search
No edit summary |
No edit summary |
||
| (14 intermediate revisions by 2 users not shown) | |||
| Line 1: | Line 1: | ||
Below you can find some common examples. ECGs can be magnified by clicking on the image.... | |||
__TOC__ | |||
{{clr}} | {{clr}} | ||
== | ==Ischemia & Myocardial Infarction== | ||
<div align="left"> | |||
[[Image:coronary_anatomy.png|thumb|300px| An overview of the coronary arteries. LM = 'Left Main' = mainstem; LAD = 'Left Anterior Descending' artery; RCX = Ramus Circumflexus; RCA = 'Right Coronary Artery'.]] | |||
<div style="width:689px"> | |||
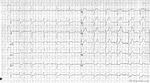
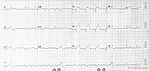
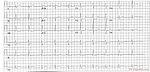
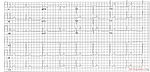
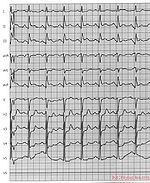
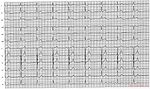
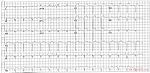
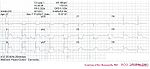
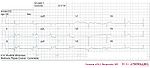
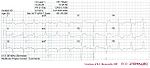
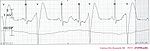
Guess the culprit coronary artery that was occluded in these examples of myocardial infarctions | |||
{{ImageC |image=ami0001.jpg |link=MI 1|text=[[MI 1]]}} | |||
{{ImageC |image=ami0002.jpg |link=MI 2|text=[[MI 2]]}} | |||
{{ImageC |image=ami0003.jpg |link=MI 3|text=[[MI 3]]}} | |||
{{ImageC |image=ami0004.jpg |link=MI 4|text=[[MI 4]]}} | |||
{{ImageC |image=ami0005.jpg |link=MI 5|text=[[MI 5]]}} | |||
{{ImageC |image=ami0006.jpg |link=MI 6|text=[[MI 6]]}} | |||
{{ImageC |image=ami0007.jpg |link=MI 7|text=[[MI 7]]}} | |||
{{ImageC |image=ami0008.jpg |link=MI 8|text=[[MI 8]]}} | |||
{{ImageC |image=ami0009.jpg |link=MI 9|text=[[MI 9]]}} | |||
{{ImageC |image=ami0010.jpg |link=MI 10|text=[[MI 10]]}} | |||
{{ImageC |image=ami0011.jpg |link=MI 11|text=[[MI 11]]}} | |||
{{ImageC |image=ami0012.jpg |link=MI 12|text=[[MI 12]]}} | |||
{{ImageC |image=ami0013.jpg |link=MI 13|text=[[MI 13]]}} | |||
{{ImageC |image=Casus2_2.jpg |link=MI 14|text=[[MI 14]]}} | |||
{{ImageC |image=AMI_anterior_LAD.jpg |link=MI 15|text=[[MI 15]]}} | |||
{{ImageC |image=KJcasus5.jpg |link=MI 16|text=[[MI 16]]}} | |||
{{ImageC |image=KJcasus6.jpg |link=MI 17|text=[[MI 17]]}} | |||
{{ImageC |image=KJcasus7.jpg |link=MI 18|text=[[MI 18]]}} | |||
{{ImageC |image=KJcasus8.jpg |link=MI 19|text=[[MI 19]]}} | |||
{{ImageC |image=KJcasus10.jpg |link=MI 20|text=[[MI 20]]}} | |||
{{ImageC |image=KJcasus12.jpg |link=MI 21|text=[[MI 21]]}} | |||
{{ImageC |image=KJcasus13.jpg |link=MI 22|text=[[MI 22]]}} | |||
{{ImageC |image=KJcasus16.jpg |link=MI 23|text=[[MI 23]]}} | |||
{{clr}} | {{clr}} | ||
</div> | |||
</div> | |||
{{clr}} | {{clr}} | ||
==Arrhythmias== | |||
== | {{ImageC |image=Casus2_2.jpg |link=Case 1|text=[[Case 1]]}} | ||
{{ImageC |image=KJcasus3.jpg |link=Case 2|text=[[Case 2]]}} | |||
{{ImageC |image=KJcasus9.jpg |link=Case 3|text=[[Case 3]]}} | |||
[[ | {{ImageC |image=Triblock.png |link=Case 4|text=[[Case 4]]}} | ||
{{ImageC |image=JJ00004.jpg |link=Case 5|text=[[Case 5]]}} | |||
{{clr}} | {{clr}} | ||
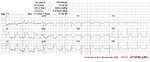
==Electrolyte Disorders== | |||
== | {{ImageC |image=KJcasu17-1.jpg |link=Case 100|text=[[Case 100]]}} | ||
{{ImageC |image=KJcasu18-3.jpg |link=Case 101|text=[[Case 101]]}} | |||
{{clr}} | {{clr}} | ||
==Miscellaneous== | |||
Click on the text below the ECG for the '''answers'''. Click on the ECG for '''enlargement of the ECG''' itself... | |||
<gallery> | <gallery> | ||
Image: | Image:RVDB1.jpg|[[Example 23]] | ||
Image:DVA0011.jpg|[[Example 24]] | |||
Image:DVA0229.jpg|[[Example 25]] | |||
Image: | |||
Image: | |||
</gallery> | </gallery> | ||
{{Box| | |||
==Advanced cases== | |||
For more advanced cases see: | |||
*[[Rhythm Puzzles]] by Prof. A.A.M. Wilde, MD, PhD | |||
*[[Case reports by W.G. De Voogt%2C MD%2C PhD]] | |||
*The ''[[De Voogt ECG Archive]]'' contains > 2000 categorized ECGs | |||
}} | |||
[[Category:Cases and Examples]] | |||
Latest revision as of 03:04, 6 June 2009
Below you can find some common examples. ECGs can be magnified by clicking on the image....
Ischemia & Myocardial Infarction




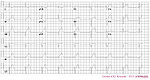






Arrhythmias



Electrolyte Disorders

Miscellaneous
Click on the text below the ECG for the answers. Click on the ECG for enlargement of the ECG itself...


Advanced cases
For more advanced cases see:
- Rhythm Puzzles by Prof. A.A.M. Wilde, MD, PhD
- Case reports by W.G. De Voogt, MD, PhD
- The De Voogt ECG Archive contains > 2000 categorized ECGs