McGill Case 4: Difference between revisions
Jump to navigation
Jump to search
No edit summary |
No edit summary |
||
| (8 intermediate revisions by the same user not shown) | |||
| Line 6: | Line 6: | ||
}} | }} | ||
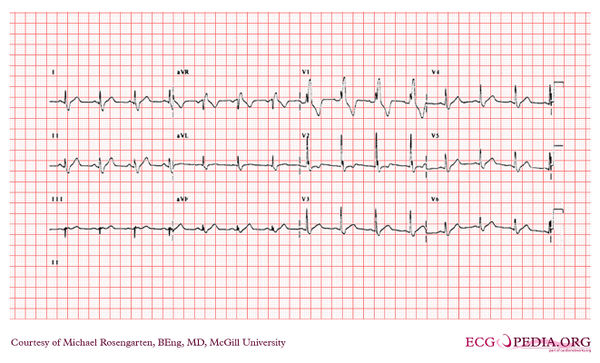
[[File: | [[File:E000704.jpg|thumb|600px|left|This cardiogram shows sinus rhythm with a normal pr interval and a prolonged QRS interval (>120ms). There is a conduction abnormality best described as a right bundle branch block due to the rsR' wave in V1. Note the S wave in V6 which is due to the RBBB is smaller than the R wave in V6. The axis of the QRS is difficult to determine, but one usually looks at the first 60 ms. (1 1/2 small squares) to determine the axis with a RBBB. If the axis of the first 60 ms. of the QRS is more than 90 degrees and there is an rS in lead I and a Q in lead III then on would consider a left posterior fasicular block. This is not the case here.]] | ||
Latest revision as of 05:07, 10 February 2012
|

This cardiogram shows sinus rhythm with a normal pr interval and a prolonged QRS interval (>120ms). There is a conduction abnormality best described as a right bundle branch block due to the rsR' wave in V1. Note the S wave in V6 which is due to the RBBB is smaller than the R wave in V6. The axis of the QRS is difficult to determine, but one usually looks at the first 60 ms. (1 1/2 small squares) to determine the axis with a RBBB. If the axis of the first 60 ms. of the QRS is more than 90 degrees and there is an rS in lead I and a Q in lead III then on would consider a left posterior fasicular block. This is not the case here.