McGill Case 268: Difference between revisions
Jump to navigation
Jump to search
(Created page with "{{McGillcase| |previouspage= McGill Case 267 |previousname= McGill Case 267 |nextpage= McGill Case 270 |nextname= McGill Case 270 }} [[File:E268.jpg|thumb|600px|left|The card...") |
No edit summary |
||
| Line 2: | Line 2: | ||
|previouspage= McGill Case 267 | |previouspage= McGill Case 267 | ||
|previousname= McGill Case 267 | |previousname= McGill Case 267 | ||
|nextpage= McGill Case | |nextpage= McGill Case 269 | ||
|nextname= McGill Case | |nextname= McGill Case 269 | ||
}} | }} | ||
Latest revision as of 21:11, 19 February 2012
|

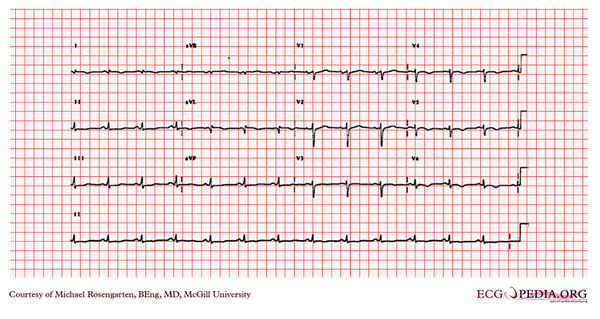
The cardiogram shows sinus rhythm and a QRS with a rightward axis, as well as wide Q waves in leads I and AVL as well as a poor r wave progression across the anterior chest leads. There is also slight ST elevation in leads I, aVL, and T wave inversion in the lateral leads. The EKG is consistent with a lateral wall myocardial infarction. The patient had had a myocardial infarction a few months before. This event was associated with a cardiac arrest due to ventricular fibrillation which was successfully treated by the 911 ambulance service.