File:E000763.jpg: Difference between revisions
No edit summary |
No edit summary |
||
| Line 1: | Line 1: | ||
== Summary == | |||
{{Information | |||
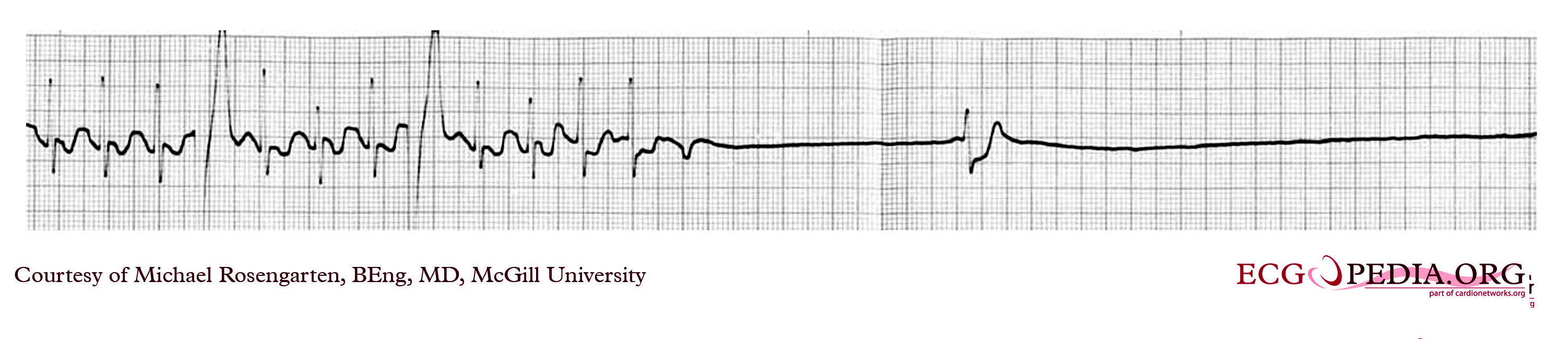
|Description = This is a rhythm strip from a 67 year old patient with mild renal failure and hypertension. He presented himself with four episodes of syncope 30-40 days apart. | |||
All episodes happened without warning, and the patient claimed that he had neither confusion nor headaches after the episodes. | |||
Monitoring in the hospital for 3 days was unrewarding. The 12 lead EKG showed only left atrial abnormality. A surface averaged ECG was considered abnormal with a QRSD of 112ms, a RMS40 of 19.8 ms and a LAS of 38.5 ms. | |||
An invasive electrophyiology test found an HV of 55-60ms, an AH of 50ms, anterograde conduction until 170/min with block in the A/V node and no change in the QRS. Retrograde conduction was to 150/min. No ventricular tachycardia was induced with three extra stimuli. Atrial flutter was induced easily, and resulted in a ventricular rate of 145/min. It terminated spontaneously once and another time with rapid atrial pacing. | |||
The patient was release from hospital and five days of Holter monitoring revealed only a slow average heart of 66/min. | |||
The patient was equipped with a loop monitor. After 38 days of monitoring his wife found him dazed in the laundry room, pressed the record button and captured a five minute rhythm segment (4 minutes before and one minute after). The strip below is part of the five minute strip. | |||
This is an interesting case of recurrent syncope the cause of which was finally diagnosed with prolonged loop monitoring. | |||
The strips above first shows atrial flutter with 2:1 block and a ventricular rate of nearly 150/min. This is followed by asystole with one nodal beat, then a ventricular escape and finally a sinus beat and a PAC. | |||
The flutter waves are best seen after the last QRS before the period of asystole. | |||
Note that the PVCS recorded during the flutter do not affect the timing of the SVT suggesting that this is not a A/V reentrant rhythm and that the ventricle is not part of a reentrant loop. | |||
There appears to be one escape VC but where were the PVCs when the patient needed them? (during the period of asystole) The answer is partly that the patient was symptomatic because there was no escape ventricular rhythm. | |||
To be symptomatic with a tachy-brady syndrome a patient needs to have a failure of an escape focus such as an A/V nodal or the ventricle escape rhythm. | |||
Confusion tends to indicate that syncope is neurologic. In this case the patient was confused and it was his partner that pushed the event button. Prolonged asystole can cause confusion and limits the usefulness of patient loop recorders, and confusion does not rule out a cardiac arrhythmia. | |||
The patient was implanted with a VVI pacer set at 50/min. and placed on Sotalol 80 m.g. P.O. B.I.D. with resolution of his symptoms. | |||
|Category = [[Case_reports_from_Michael_Rosengarten|Case reports by Michael Rosengarten]] | |||
|Source = EKG World Encyclopedia http://cme.med.mcgill.ca/php/index.php , courtesy of Michael Rosengarten BEng, MD.McGill | |||
|Date = 2012 | |||
|Author = Michael Rosengarten BEng, MD.McGill | |||
|Permission = {{by-nc-sa-3.0}} | |||
|other_versions = None | |||
}} | |||
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Latest revision as of 00:54, 15 February 2012
Summary
| Description |
This is a rhythm strip from a 67 year old patient with mild renal failure and hypertension. He presented himself with four episodes of syncope 30-40 days apart. All episodes happened without warning, and the patient claimed that he had neither confusion nor headaches after the episodes. Monitoring in the hospital for 3 days was unrewarding. The 12 lead EKG showed only left atrial abnormality. A surface averaged ECG was considered abnormal with a QRSD of 112ms, a RMS40 of 19.8 ms and a LAS of 38.5 ms. An invasive electrophyiology test found an HV of 55-60ms, an AH of 50ms, anterograde conduction until 170/min with block in the A/V node and no change in the QRS. Retrograde conduction was to 150/min. No ventricular tachycardia was induced with three extra stimuli. Atrial flutter was induced easily, and resulted in a ventricular rate of 145/min. It terminated spontaneously once and another time with rapid atrial pacing. The patient was release from hospital and five days of Holter monitoring revealed only a slow average heart of 66/min. The patient was equipped with a loop monitor. After 38 days of monitoring his wife found him dazed in the laundry room, pressed the record button and captured a five minute rhythm segment (4 minutes before and one minute after). The strip below is part of the five minute strip.
|
|---|---|
| Category | |
| Source |
EKG World Encyclopedia http://cme.med.mcgill.ca/php/index.php , courtesy of Michael Rosengarten BEng, MD.McGill |
| Date |
2012 |
| Author |
Michael Rosengarten BEng, MD.McGill |
| Permission |
Creative Commons Attribution Noncommercial Share-Alike License |
File history
Click on a date/time to view the file as it appeared at that time.
| Date/Time | Thumbnail | Dimensions | User | Comment | |
|---|---|---|---|---|---|
| current | 00:51, 15 February 2012 | 3,004 × 649 (711 KB) | DarrelC (talk | contribs) |
{kind=link}
You cannot overwrite this file.
File usage
The following page uses this file:
{kind=link}