Clinical Disorders
| Author(s) | I.A.C. van der Bilt, MD | |
| Moderator | T.T. Keller | |
| Supervisor | ||
| some notes about authorship | ||
Medication
Digoxin

ECG changes typical for digoxin intoxication (digoxin = Lanoxin) are:
- Oddly shaped ST-depression.
- T wave flat, negative or biphasic
- Short QT interval
- Increased u-wave amplitude
- Prolonged PR-interval
- Bradyarrhythmias:
- Sinus bradycardia
- AV block. Including complete AV block and Wenkebach.
- Tachyarrhythmias:
- Junctional tachycardia
- Atrial tachycardia
- Ventricular ectopia, bigemini, monomorphic ventricular tachycardia, bidirectional ventricular tachycardia
Intoxication can lead to an SA-block or AV-block, sometimes in combination with tachycardia. NB these effects are increased by hypokalemia. In extreme high concentrations rhythm disturbances (ventricular tachycardia, ventricular fibrillation, atrial fibrillation) may develop.
Antiarrhythmics
- Anti-arrhythmics: These may lead to several ECG-changes;
- Broad and irregular P-wave
- Broad QRS complex
- Prolonged QT interval (brady-, tachycardia, AV-block, ventricular tachycardia)
- Prominent U-wave
- In case of intoxication, the above mentioned characteristics are more prominent
Additionally, several arrhthytmias can be seen.
Nortriptyline intoxication
|
|


Amitriptyline intoxication


Pericarditis
Myocarditis
Myocarditis is an inflammation of the myocardium and the interstitium. The symptoms are faint chest pain, abnormal heart rate and progressive heart failure. It can be caused by several factors: viruses, bacteria, fungi, parasites, spirochetes, auto-immune reactions, borreliosis (Lyme's disease) and HIV/AIDS.
Acute peri/myocarditis causes nonspecific ST segment changes. These can be accompanied by supraventricular and ventricular rhythm disturbances and T-wave abnormalities.
Pulmonary embolism
See the chapter Pulmonary Embolism
Chronic pulmonary disease pattern
The ECG shows low voltage QRS complexes in leads I, II, and III and a right axis deviation. This is caused by the increased pressure on the right chamber. This leads to right ventricular hypertrophy.
Pacemaker
See the chapter Pacemaker
Tamponade

In case of tamponade, fluid collects in the pericardium. Because the pericardium is stiff, the heart is compressed, resulting in filling difficulties. This is a potentially life-threatening situation and should be treated with pericardiocentesis, drainage of the fluid. Tamponade can be the result of pericarditis or myocarditis. After a myocardial infarction a tamponade can also develop; this is called Dresslers' Syndrome. In case of cancer,increased pericardial fluid may develop. This is usually caused by pericarditis carcinomatosis, meaning that the cancer has spread to the pericardium
The ECG shows:
- Sinus tachycardia
- Low-voltage QRS complexes microvoltages
- Alternation of the QRS complexes, usually in a 2:1 ratio. Electrical alternans can also be seen in myocardial ischemia, acute pulmonary embolism, and tachyarrhythmias
- PR segment depression (this can also be observed in an atrial infarction)
Ventricular Aneurysm
The ECG pattern suggests an acute MI. All classical signs of MI may occur:; Q waves, ST segment elevations (>1mm, >4 weeks present)and T wave inversions are present. To exclude an acute MI, comparison with old ECG's is compulsory (MI has occurred years before).
Dilated Cardiomyopathy
Often, a LBBB or broadened QRS-complex can be seen. Additionally, nonspecific ST segment changes are present with signs of left atrial enlargement.
Hypertrophic Obstructive Cardiomyopathy
A HOCM is a hereditary illness. On the ECG there are signs of left ventricular hypertrophy and left atrial enlargement.
Electrolyte disturbances
See chapter: electrolyte disturbances
Hypothermia

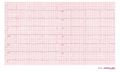
A 12 lead ECG of a patient with a body temperature of 32 degrees Celsius. Note the sinus bradycardia, the prolonged QT interval (QTc is not prolonged) and the Osborne J wave, most prominently in leads V2-V5
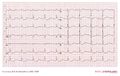
An ECG of a patient with a body temperature of 28 degrees Celsius.


In hypothermia a number of specific changes can be seen;[1]
- Sinus bradycardia
- Prolonged QTc-interval
- ST segment elevation (inferior and left precordial leads)
- Osborne-waves (slow deflections at the end of the QRS-complex)
ECG changes after neurologic events

In 1938, Aschenbrenner [2] noted that repolarization abnormalities may occur after increased intracranial pressure. Since then, many publications have described ECG changes after acute neurological events.
ECG changes that may occur are:
- Q waves
- ST segment elevations,
- ST segment depressions,
- T wave changes. Large negative T waves over the precordial leads are observed frequently.
- Prolonged QT-interval.
- Prominent u-waves.
These abnormalities are frequently seen after subarachnoid_hemorrhage (SAH) (if measured serially, almost every SAH patients has at least one abnormal ECG.), but also in subdural hematoma, ischemic CVA's, brain Tumors, Guillain Barré, epilepsy and migraine. The ECG changes are generally reversible and have limited prognostic value. However, the ECG changes can be accompanied with myocardial damage and echocardiographic changes. The cause of the ECG changes is not yet clear. The most common hypothesis is that of a neurotramitter "catecholamine storm" caused by sympathetic stimulation.
Cardiac contusion
Cardiac contusion (in latin: contusio cordis or commotio cordis) is caused by a blunt trauma to the chest, often caused by a car or motorbike accident or in martial arts[3]. Rhythm disturbances and even heart failure can occur. Diagnosis is made using echocardiography and laboratory testing for cardiac enzymes. Possible ECG changes are:[4]
Not-specific changes
- Pericarditis-like ST elevation or PTa depression
- Prolonged QT interval
Myocardial damage
- New Q waves
- ST-T segment elevation or depression
Conduction delay
- Right bundle branch block
- Fascicular blok
- AV delay(1st, 2nd, and 3rd degree AV blok)
Arrhythmias
- Sinus tachycardia
- Atrial and ventricular extrasystoles
- Atrial fibrillation
- Ventricular tachycardia
- Ventricular fibrillation
- Sinus bradycardia
- Atrial tachycardia
Lown Ganong Levine Syndrome
The Lown Ganong Levine Syndrome is a pre-excitation syndrome in which the atria are connected to the lower part of the AV node or bundle of His. On the ECG:
- Short PR interval, < 120 ms
- Normal QRS complex
- No delta wave
Left and right bundle branch block
See: Conduction delay
Cocaine Intoxication
|
References
- Solomon A, Barish RA, Browne B, and Tso E. The electrocardiographic features of hypothermia. J Emerg Med. 1989 Mar-Apr;7(2):169-73. DOI:10.1016/0736-4679(89)90265-5 |
-
Aschenbrenner R, Bodechtel G, Ãber Ekg.-Veränderungen bei Hirntumorkranken. Journal of Molecular Medicine, 17, 9, 2/1/1938, Pages 298-302, http://dx.doi.org/10.1007/BF01778563
- Ashrafian H. Sudden death in young athletes. N Engl J Med. 2003 Dec 18;349(25):2464-5; author reply 2464-5. DOI:10.1056/NEJM200312183492518 |
- Sybrandy KC, Cramer MJ, and Burgersdijk C. Diagnosing cardiac contusion: old wisdom and new insights. Heart. 2003 May;89(5):485-9. DOI:10.1136/heart.89.5.485 |
- Rodger M, Makropoulos D, Turek M, Quevillon J, Raymond F, Rasuli P, and Wells PS. Diagnostic value of the electrocardiogram in suspected pulmonary embolism. Am J Cardiol. 2000 Oct 1;86(7):807-9, A10. DOI:10.1016/s0002-9149(00)01090-0 |
- Ferrari E, Imbert A, Chevalier T, Mihoubi A, Morand P, and Baudouy M. The ECG in pulmonary embolism. Predictive value of negative T waves in precordial leads--80 case reports. Chest. 1997 Mar;111(3):537-43. DOI:10.1378/chest.111.3.537 |