Chamber Hypertrophy and Enlargment
| Author(s) | J.S.S.G. de Jong | |
| Moderator | J.S.S.G. de jong | |
| Supervisor | ||
| some notes about authorship | ||
In hypertrophy the heart muscle becomes thicker. This can have different causes. Left ventricular hypertrophy results from an increase in left ventricular workload, e.g., during hypertension or aortic valve stenosis. Right ventricular hypertrophy results from an increase in right ventricular workload, e.g., emphysema or pulmonary embolization. These causes are fundamentally different from hypertrophic obstructive cardiomyopathy (HCM), which is a congenital misalignment of cardiomyocytes resulting in hypertrophy.
Left and right ventricular hypertrophy can be distinguished on the ECG:
Left ventricular hypertrophy


As the left ventricular wall becomes thicker, the QRS complexes become larger. This is especially true for leads V1-V6. The S wave in V1 is deep, the R wave in V4 is high. Often some ST depression can be seen in leads V5-V6, which is in this setting is called a 'strain pattern'.
To diagnose left ventricular hypertrhophy on the ECG one of the following criteria should be met: The Sokolow-Lyon criterium[1]), this is most often used:
- R in V5 or V6 + S in V1 >35 mm.
Other criteria:
- R >26 mm in V5 or V6;
- R >20 mm in I, II or III;
- R >12 mm in aVL (in the absence of left anterior fascicular block);
The Cornell-criterium has different values in men and women:
- R in aVL and S in V3 >28 mm in men
- R in aVL and S in V3 >20 mm in women
In the Romhilt-Estes Score LVH is likely with 4 or more points. LVH is present with 5 or more points:
- Amplitude of R or S wave in limb leads >2.0 mV, or S wave in V1 or V2 >3.0 mV, or R wave in V5 or V6 >3.0 mV = 3 points.
- ST-segment changes with or without digitalis = 1 or 2 points, respectively.
- LA abnormality = 3 points.
- Left-axis deviation -30° or more = 2 points.
- QRS duration >90 ms = 1 point.
- Intrinsicoid deflection in V5 or V6 = 0.05 to 0.07 s.
Left ventricular hypertrophy has prognostic consequences as has been found in several studies.[2][3]
Example
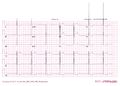
ECG of patient with left ventricular hypertrophy according to the Sokolow-Lyon criteria

Another example of extreme left ventricular hypertrophy in a patient with severe aortic valve stenosis.

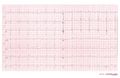
ECG of a patient with LVH and subendocardial ischemia leading to positive cardiovascular markers in blood testing.



Right ventricular hypertrophy


Right ventricular hypertrophy occurs mainly in lung disease or in congenital heart disease. The ECG shows a negative QRS complex in I (and thus a right heart axis) and a positive QRS complex in V1.
- QRS duration < 120ms
- Right heart axis (> 110 degrees)
- Dominant R wave:
- R/S ratio in V1 or V3R > 1, or R/S ratio in V5 or V6 <= 1
- R wave in V1 >= 7 mm
- R wave in V1 + S wave in V5 or V6 > 10.5 mm
- rSR= in V1 with R'= > 10 mm
- qR complex in V1
- Secondary ST-T changes in right precordial leads
- Right atrial abnormality
- Onset of intrinsicoid deflection in V1 between 0.035 and 0.055 s
Left atrial enlargement

Left atrial enlargement

Left atrial enlargement with ECG.

Left atrial enlargement as seen in lead V1.
Left atrial enlargement as seen on a 12 lead ECG




- Criteria for left atrial voor left atrial enlargement. Either
- P wave with a broad (>0.04 sec or 1 small square) and deeply negative (>1 mm) terminal part in V1
- P wave duration >0.12 sec in leads I and / or II
Left atrial enlargement is often seen in mitral valve insufficiency, resulting in back flow of blood from the left ventricle to the left atrium and subsequent increased local pressure.
Right atrial enlargement

Right atrial enlargement

Right atrial enlargement


- Right atrial enlargement is defined as either
- P >2,5 mm in II / III and / or aVF
- P >1,5 mm in V1.
Right atrial enlargement can result from increased pressure in the pulmonary artery, e.g. after pulmonary embolization. A positive part of the biphasic p-wave in lead V1 larger than the negative part indicates right atrial enlargement. The width of the p wave does not change.
Biatrial enlargement
- Biatrial enlargement
- Biphasic p wave in V1 of more than 0.04 sec duration. The positive initial part is > 1.5mm and the negative terminal part > 1mm
In biatrial enlargement the ECG shows signs of both left and right atrial enlargement. In V1 the p wave has large peaks first in a positive and later in a negative direction.
References
-
Sokolow M, Lyon TP: The ventricular complex in left ventricular hyptertrophy as obtained by unipolar precordial and limb leads. Am Heart J 37: 161, 1949
- Sundström J, Lind L, Arnlöv J, Zethelius B, Andrén B, and Lithell HO. Echocardiographic and electrocardiographic diagnoses of left ventricular hypertrophy predict mortality independently of each other in a population of elderly men. Circulation. 2001 May 15;103(19):2346-51. DOI:10.1161/01.cir.103.19.2346 |
- Levy D, Salomon M, D'Agostino RB, Belanger AJ, and Kannel WB. Prognostic implications of baseline electrocardiographic features and their serial changes in subjects with left ventricular hypertrophy. Circulation. 1994 Oct;90(4):1786-93. DOI:10.1161/01.cir.90.4.1786 |