Brugada Syndrome
| Author(s) | P.G. Postema, MD | |
| Moderator | P.G. Postema, MD | |
| Supervisor | ||
| some notes about authorship | ||
The Brugada syndrome is an hereditary disease that is associated with higher risk of sudden cardiac death. It is characterized by typical ECG abnormalities: ST segment elevation in the precordial leads (V1 - V3).




Characteristics of the Brugada syndrome:
- Inheritable arrhythmia syndrome with autosomal dominant inheritance. If one of both parents is affected, their children (either males or females) have a 50% chance of inheriting the disease.
- Males are more often symptomatic than females, probably by the influence of sex hormones on cardiac arrhythmias and/or ion channels, and a different distribution of ion channels across the heart in males versus females.
- The arrhythmias usually occur between 30 and 40 years of age. (range 1-77 yrs) and often during rest or while sleeping (high vagal tone).
- Only in about 30% of patients, genetic defects can be detected in the (SCN5A) gene which encodes the cardiac sodium channel (loss-of-function mutation). In much smaller quantities mutations may be found in the GPD1L gene (which probably influences cardiac sodium channel function) or in cardiac calcium channel encoding genes (CACNxxx). In the other patients, the disease is probably multi-genetic or caused by yet unknown genetic defects.
- The right ventricle is most affected in Brugada syndrome, and particularly (but not specifically) the right ventricular outflow tract .
- The prevalence varies between 5-50:10.000, largely depending on geographic location. In some south-east Asian countries the disease is considered endemic and believed to be the second cause of death amongst young men (after car accidents). In these countries Brugada syndrome is believed to underly (in part) the 'Sudden Unexpected Death Syndrome' (SUDS). This relation has however not been thoroughly investigated and there are almost no epidemiological studies into Brugada syndrome ECGs (apart from Japan). In different Asian countries, different names have been given to SUDS: in the Phillipines it is called bangungut (to rise and moan in sleep) and in Thailand lai tai (death during sleep).
The Brugada brothers were the first to describe the characteristic ECG findings and link them to sudden death. Before that, the characteristic ECG findings, were often mistaken for a right ventricle myocardial infarction and already in 1953, a publication mentions that the ECG findings were not associated with ischemia as people often expected.[2]
Diagnosis and treatment
- Patients who are symptomatic (unexplained syncope, ventricular tachycardias or survivors of sudden cardiac death) have a mortality risk of up to 10% per year. In these patients an ICD is adviced to be implanted.
- Some groups advice an electrophysiological investigation (inducibility of VF) for risk assessment in Brugada patients,[3][4] but others could not reproduce the predictive value of these tests,[5][6] so the value of inducibility is (very) controversial.
- In large studies familial sudden death did not appear to be a risk factor for sudden death in siblings.
- In asymptomatic patients in whom the Brugada ECG characteristics are present (either spontaneously or provoked by fever or sodium channel blockers like ajmaline, procainimde or flecainide) life style advices are given, which include:
- A number of medications should not be taken (amongst which beta-blockers, and sodium channel blockers such as certain anti-depressants and anti-arrhythmics)
- Rigorous treatment of fever with paracetamol / Tylenol, as fever may elicited the Brugada ECG and arrhythmias in some patients.
- Spontaneous Type I ECGs do however appear to be more prevalent in patients who experienced symptoms.
For a full list of the diagnostic criteria, see [7]
Electrocardiographic criteria

Three ECG repolarization patterns in the right precordial leads are recognized in the diagnosis of Brugada syndrome.
Type I is the only ECG criterion that is diagnostic of Brugada syndrome. The type I ECG is characterized by a J elevation >=2 mm (0.2 mV) a coved type ST segment followed by a negative T wave (see figure). Brugada syndrome is definitively diagnosed when a type 1 ST-segment is observed in >1 right precordial lead (V1 to V3) in the presence or absence of a sodium channel–blocking agent, and in conjunction with one of the following:
- documented ventricular fibrillation (VF)
- polymorphic ventricular tachycardia (VT)
- a family history of sudden cardiac death at <45 years old
- coved-type ECGs in family members
- inducibility of VT with programmed electrical stimulation
- syncope
- nocturnal agonal respiration.
The sensitivity of the ECG for Brugada syndrome can be increased with placement of ECG leads in the intercostal space above V1 and V2 (V1ic3 and V2ic3)
Electrocardiograms of Brugada patients can change over time from type I to type II and/or normal ECGs and back. A type III ECG is rather common and is considered a normal variant, but also the Type II is a normal variant (albeit suggestive of Brugada syndrome).
| Type I | Type II | Type III | |
|---|---|---|---|
| J wave amplitude | >= 2mm | >= 2mm | >= 2mm |
| T wave | negative | positive or biphasis | positive |
| ST-T configuration | coved type | saddleback | saddleback |
| ST segment (terminal portion) | gradually descending | elevated >= 1mm | elevated < 1mm |
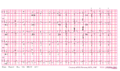
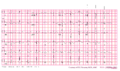
- Examples of Brugada syndrome type I




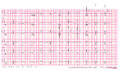
Brugada ECG during ajmaline testing






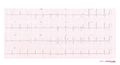
- Examples of Brugada syndrome type II


External links
- Cardiogenetics website of the AMC cardiogentica.nl
- Brugada.org
- Genereview Brugada
Referenties
- Brugada P and Brugada J. Right bundle branch block, persistent ST segment elevation and sudden cardiac death: a distinct clinical and electrocardiographic syndrome. A multicenter report. J Am Coll Cardiol. 1992 Nov 15;20(6):1391-6. DOI:10.1016/0735-1097(92)90253-j |
- OSHER HL and WOLFF L. Electrocardiographic pattern simulating acute myocardial injury. Am J Med Sci. 1953 Nov;226(5):541-5.
- Brugada J, Brugada R, Antzelevitch C, Towbin J, Nademanee K, and Brugada P. Long-term follow-up of individuals with the electrocardiographic pattern of right bundle-branch block and ST-segment elevation in precordial leads V1 to V3. Circulation. 2002 Jan 1;105(1):73-8. DOI:10.1161/hc0102.101354 |
- Brugada P, Brugada R, Mont L, Rivero M, Geelen P, and Brugada J. Natural history of Brugada syndrome: the prognostic value of programmed electrical stimulation of the heart. J Cardiovasc Electrophysiol. 2003 May;14(5):455-7. DOI:10.1046/j.1540-8167.2003.02517.x |
- Priori SG, Napolitano C, Gasparini M, Pappone C, Della Bella P, Giordano U, Bloise R, Giustetto C, De Nardis R, Grillo M, Ronchetti E, Faggiano G, and Nastoli J. Natural history of Brugada syndrome: insights for risk stratification and management. Circulation. 2002 Mar 19;105(11):1342-7. DOI:10.1161/hc1102.105288 |
- Eckardt L, Probst V, Smits JP, Bahr ES, Wolpert C, Schimpf R, Wichter T, Boisseau P, Heinecke A, Breithardt G, Borggrefe M, LeMarec H, Böcker D, and Wilde AA. Long-term prognosis of individuals with right precordial ST-segment-elevation Brugada syndrome. Circulation. 2005 Jan 25;111(3):257-63. DOI:10.1161/01.CIR.0000153267.21278.8D |
- Antzelevitch C, Brugada P, Borggrefe M, Brugada J, Brugada R, Corrado D, Gussak I, LeMarec H, Nademanee K, Perez Riera AR, Shimizu W, Schulze-Bahr E, Tan H, and Wilde A. Brugada syndrome: report of the second consensus conference. Heart Rhythm. 2005 Apr;2(4):429-40. DOI:10.1016/j.hrthm.2005.01.005 |
- Wilde AA, Antzelevitch C, Borggrefe M, Brugada J, Brugada R, Brugada P, Corrado D, Hauer RN, Kass RS, Nademanee K, Priori SG, Towbin JA, and Study Group on the Molecular Basis of Arrhythmias of the European Society of Cardiology. Proposed diagnostic criteria for the Brugada syndrome: consensus report. Circulation. 2002 Nov 5;106(19):2514-9. DOI:10.1161/01.cir.0000034169.45752.4a |