Approach to the Wide Complex Tachycardia: Difference between revisions
Jump to navigation
Jump to search
mNo edit summary |
|||
| Line 6: | Line 6: | ||
== Brugada criteria == | == Brugada criteria == | ||
{| class="wikitable" width="500px" | {| class="wikitable" width="500px" | ||
! colspan="3" |Brugada criteria | ! colspan="3" |Brugada criteria to differentiate [[SVT]] from [[VT]] <cite>Brug1</cite> | ||
|- | |- | ||
| | | Are there fusion or capture beats? (this is not an item from Brugada, it is however very specific|| Yes? => VT || specificy=100% [[image:fusionbeat.png|thumb|100px]] | ||
|- | |- | ||
| RS complexen | | RS complexen missing in the chest leads? || Yes? => [[VT]] || sensitivity=21% specificity=100% | ||
|- | |- | ||
| RS-interval in | | RS-interval in one of the cheast leads > 100 msec (in the absence of anti-arrhythmics)? || Yes? => VT || sensitivity=66% specificity=98% | ||
|- | |- | ||
| | | [[AV-dissociation]]? || Yes? => probably [[VT]] (Note [[AVNRT]] can also present with AV dissociation!)|| sensitivity=82% specifity=98% | ||
|- | |- | ||
! colspan="3" | | ! colspan="3" | Morphological criteria (if the above criteria are inconclusive) | ||
|- | |- | ||
!colspan="3" |[[ | !colspan="3" |[[LBBB]] pattern | ||
|- | |- | ||
| | | Initial R more than 40ms? ||Yes => VT || [[Image:Rhythm_RSratio.png|thumb|100px]] | ||
|- | |- | ||
| Slurred of | | Slurred or notched downwards leg of S wave in leads V1 or V2 || Yes => [[VT]] || | ||
|- | |- | ||
| | | Beginning of Q to nadir QS >60 ms in V1 or V2? || Yes => [[VT]] || LR >50:1 | ||
|- | |- | ||
| Q | | Q or QS in V6? || Yes => [[VT]] || LR >50:1 | ||
|- | |- | ||
| colspan="3" |[[Image:Rhythm_LBTBmorph_en.png|thumb|300px]] | | colspan="3" |[[Image:Rhythm_LBTBmorph_en.png|thumb|300px]] | ||
|- | |- | ||
! colspan="3" |[[ | ! colspan="3" |[[RBBB]] pattern | ||
|- | |- | ||
| | | Monofasic R or qR in V1? ||Yes => [[VT]] || | ||
|- | |- | ||
| R | | R taller than R' (rabbit-ear sign)?||Yes => [[VT]] || LR >50:1 | ||
|- | |- | ||
| rS in V6? || | | rS in V6? || Yes => VT || LR >50:1 | ||
|- | |- | ||
| colspan="3" |[[Image:Rhythm_RBTBmorph_en.png|thumb|300px]] | | colspan="3" |[[Image:Rhythm_RBTBmorph_en.png|thumb|300px]] | ||
| Line 43: | Line 43: | ||
{{clr}} | {{clr}} | ||
== | ==Examples== | ||
<gallery> | <gallery> | ||
Image:wide_qrs_tachy_AAM1.jpg| | Image:wide_qrs_tachy_AAM1.jpg|Wide complex tachycardia. No AV dissociation. RBBB. Resembles sinus rhythm from the same patient. Conclusio SVT with [[RBBB]] | ||
Image:wide_qrs_tachy_AAM2.jpg|ECG | Image:wide_qrs_tachy_AAM2.jpg|ECG from the same patient in sinus rhythm. The QRS complex is very similiar. | ||
Image:wide_qrs_tachy_AAM3.png| | Image:wide_qrs_tachy_AAM3.png|Wide complex tachycardia. LBBB configuration. Absence of RS in the chest leads. [[AV dissociation]] is present. Conclusion: [[VT]] | ||
Image:wide_qrs_tachy_AAM4.png| | Image:wide_qrs_tachy_AAM4.png|Wide complex tachycardia. LBBB configuration. Absence of RS in the chest leads. [[AV dissociation]] is present. Conclusion: [[VT]]`ß | ||
</gallery> | </gallery> | ||
== Referenties == | == Referenties == | ||
Revision as of 14:05, 11 November 2009
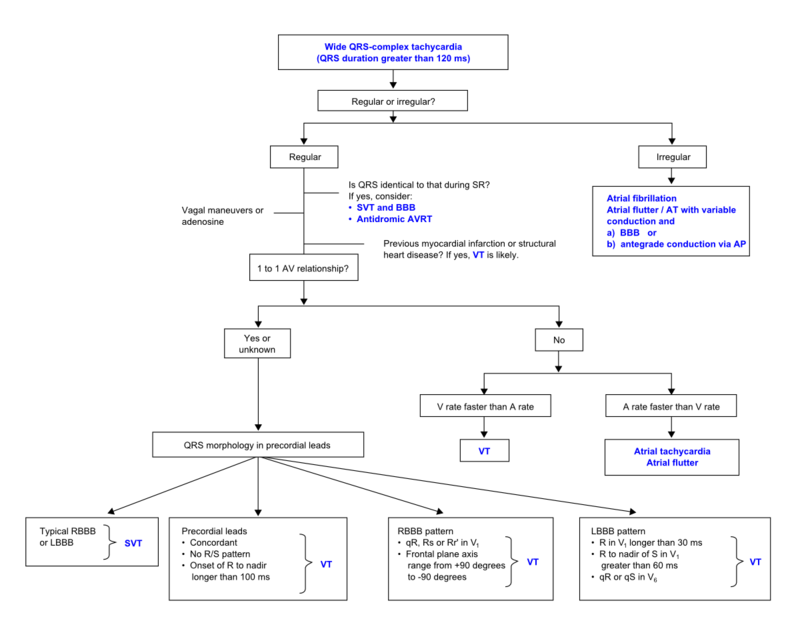
During wide complex tachycardia (heart rate > 100/min, QRS > 0.12 sec) the differentiation between supraventricular and ventricular origin of the arrhythmia is important to guide therapy. Several algorhythms have been developed to aid in this differentiation.
The ACC algorhythm [1]

SVT vs VT algorhytm. Adapted from [1]
Brugada criteria
| Brugada criteria to differentiate SVT from VT [2] | ||
|---|---|---|
| Are there fusion or capture beats? (this is not an item from Brugada, it is however very specific | Yes? => VT | specificy=100% |
| RS complexen missing in the chest leads? | Yes? => VT | sensitivity=21% specificity=100% |
| RS-interval in one of the cheast leads > 100 msec (in the absence of anti-arrhythmics)? | Yes? => VT | sensitivity=66% specificity=98% |
| AV-dissociation? | Yes? => probably VT (Note AVNRT can also present with AV dissociation!) | sensitivity=82% specifity=98% |
| Morphological criteria (if the above criteria are inconclusive) | ||
| LBBB pattern | ||
| Initial R more than 40ms? | Yes => VT | |
| Slurred or notched downwards leg of S wave in leads V1 or V2 | Yes => VT | |
| Beginning of Q to nadir QS >60 ms in V1 or V2? | Yes => VT | LR >50:1 |
| Q or QS in V6? | Yes => VT | LR >50:1 |
| RBBB pattern | ||
| Monofasic R or qR in V1? | Yes => VT | |
| R taller than R' (rabbit-ear sign)? | Yes => VT | LR >50:1 |
| rS in V6? | Yes => VT | LR >50:1 |

Examples
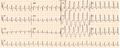
Wide complex tachycardia. No AV dissociation. RBBB. Resembles sinus rhythm from the same patient. Conclusio SVT with RBBB
ECG from the same patient in sinus rhythm. The QRS complex is very similiar.
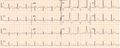
Wide complex tachycardia. LBBB configuration. Absence of RS in the chest leads. AV dissociation is present. Conclusion: VT
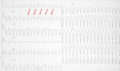
Wide complex tachycardia. LBBB configuration. Absence of RS in the chest leads. AV dissociation is present. Conclusion: VT`ß


{kind=link}
{kind=link}
{kind=link}
Referenties
- Blomström-Lundqvist C, Scheinman MM, Aliot EM, Alpert JS, Calkins H, Camm AJ, Campbell WB, Haines DE, Kuck KH, Lerman BB, Miller DD, Shaeffer CW, Stevenson WG, Tomaselli GF, Antman EM, Smith SC Jr, Alpert JS, Faxon DP, Fuster V, Gibbons RJ, Gregoratos G, Hiratzka LF, Hunt SA, Jacobs AK, Russell RO Jr, Priori SG, Blanc JJ, Budaj A, Burgos EF, Cowie M, Deckers JW, Garcia MA, Klein WW, Lekakis J, Lindahl B, Mazzotta G, Morais JC, Oto A, Smiseth O, Trappe HJ, and European Society of Cardiology Committee, NASPE-Heart Rhythm Society. ACC/AHA/ESC guidelines for the management of patients with supraventricular arrhythmias--executive summary. a report of the American college of cardiology/American heart association task force on practice guidelines and the European society of cardiology committee for practice guidelines (writing committee to develop guidelines for the management of patients with supraventricular arrhythmias) developed in collaboration with NASPE-Heart Rhythm Society. J Am Coll Cardiol. 2003 Oct 15;42(8):1493-531. DOI:10.1016/j.jacc.2003.08.013 |
- Brugada P, Brugada J, Mont L, Smeets J, and Andries EW. A new approach to the differential diagnosis of a regular tachycardia with a wide QRS complex. Circulation. 1991 May;83(5):1649-59. DOI:10.1161/01.cir.83.5.1649 |