AVNRT
| This is part of: Supraventricular Rhythms |
| {{{locatieafbeelding}}} | |
| Atrial rate | 180-250 bpm |
| Ventricular rate | 180-250 bpm |
| Regularity | regular |
| Origin | AV node |
| P-wave | inside or right after the QRS complex |
| Effect of adenosine | terminates the arrhythmia(!) |
| Example ECG: {{{example}}} | |
| Example ECG2: {{{example2}}} | |
AV Nodal Re-entry Tachycardia (AVNRT) or Atrial-Ventricular Nodal Re-entry Tachycardia is a supra-ventricular arrhythmia, and more precisely, a nodal arrhythmia. AVNRT is the most frequently occurring form of regular tachycardia. More females than males have signs of AVNRT. The ratio is approximately 3:1. Symptoms are bouts of fast heart rates with sudden onset. Neck vein palpitations can be prominent (the 'Frog Sign'). Termination is often possible with valsalva manouevres (blowing on wrist, squatting, carotid sinus massage) or medication (adenosine, verapamil, diltiazem), or electrocardioversion. An AVNRT is a regular rhythm with a rate of 180-250 /min. A condition for AVNRT to occur is that 2 electric pathways occur in and around the AV node (a slow paced and a fast paced pathway). That gives way to the ccurrence of re-entry.

Two forms of ANVRT occur: typical and atypical ANVRT
- Typical ANVRT (also described as common ANVRT or slow-fast ANVRT): The impulse travels over the slow pathway towards the ventricles and returns via the fast pathway to the atria. The retrograde P wave (or Atrial echo) shows up at the end of the QRS. 90 % of all patients with ANVRT are diagnosed with typical ANVRT. Spontaneous termination of typical AVNRT often occurs in the fast pathway (terminates with a QRS on the ECG), induced termination with carotid sinus massage or adenosine results in termination in the slow pathway (terminates with retrograde P on ECG).
- Atypical ANVRT (also described as uncommon ANVRT or fast-slow ANVRT): The impulse travels via the fast pathway towards the ventricles and returns via the slow pathway to the atria. The retrograde P wave appears far behind the QRS. Only about 6% of all ANVRT patients are diagnosed with atypical ANVRT.
The remaining cases of ANVRT patients are diagnosed with a form of ANVRT that is even more rare. This form of ANVRT is slow/slow ANVRT (The impulse follows a complex route through the AV node and the surrounding area). Only 4 % of all patients diagnosed with ANVRT have slow/slow ANVRT.
How does an ANVRT show up on an ECG?
Two sensitive characteristics to identify AVNRT on the ECG are:
- R'. This is a small secondary R wave. It resembles a right bundle branch block, but the QRS width stays < 120ms.
- RP << 100ms. The distance between the R and P waves is less than 100ms.
- Onset after a premature atrial beat with delayed conduction to the ventricles.
Examples
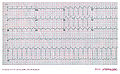
Another example of AV nodal re-entry tachycardia
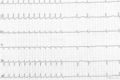
AV Nodal Re-entry Tachycardia (AVNRT) terminated by adenosine injection. Note that the last complex of the tachycardia has a retrograde P wave.

AV Nodal Re-entry Tachycardia (AVNRT)


