Approach to the Wide Complex Tachycardia
During wide complex tachycardia (heart rate > 100/min, QRS > 0.12 sec) the differentiation between supraventricular and ventricular origin of the arrhythmia is important to guide therapy. Several algorithms have been developed to aid in this differentiation (below). It is important to keep in mind that a good estimate of VT versus SVT can be made based on the clinical vignette:
- 'Horizontal entrance' into the ER. Older patient with previous myocardial infarction = most likely VT
- Younger patient with known paroxysmal tachycardias and who is hemodynamically stable = most like SVT
The ACC algorithm [1]
ECG algorithms to differentiate wide QRS-complex tachycardias
Several ECG algorithms have been developed to differentiate wide QRS-complex tachycardias. Most of them performed very well in the population they were based upon. A recent review tested five commonly used algorithms in a control population and found that each of them only performed reasonably well in differentiating VT from SVT (accuracy 66-77%).[2] The five criteria tested were:
- Brugada algorithm (below).[3] This is the most commonly used algorithm. SN 89%, SP 59.2%.
- The lead II R-wave-peak-time (below). [4] Sensitivity 60%, specificity 82.7%.
- The aVR algorithm (below). [5] Sensitivity 87.1%, specificity 48%.
- The Bayesian algorithm.[6] This calculates a score based on 19 morpologic features. Sensitivity 89%, specificity 52%.
- The Griffith algorithm (below).[7] Sensitivity 94.2%, specificity 39.8%.
Brugada algorithm

| Morphological criteria (if the above criteria are inconclusive) | ||
|---|---|---|
| LBBB pattern | ||
| Initial R more than 40ms? | Yes => VT | |
| Slurred or notched downwards leg of S wave in leads V1 or V2 | Yes => VT | |
| Beginning of Q to nadir QS >60 ms in V1 or V2? | Yes => VT | LR >50:1 |
| Q or QS in V6? | Yes => VT | LR >50:1 |
| RBBB pattern | ||
| Monofasic R or qR in V1? | Yes => VT | |
| R taller than R' (rabbit-ear sign)? | Yes => VT | LR >50:1 |
| rS in V6? | Yes => VT | LR >50:1 |



Ultrasimple Brugada criterion: RW to peak Time (RWPT)

In 2010 Joseph Brugada et al. published a new criterion to differentiate VT from SVT in wide complex tachycardias: the R wave peak time in Lead II [4]. They suggest measuring the duration of onset of the QRS to the first change in polarity (either nadir Q or peak R) in lead II. If the RWPT is ≥ 50ms the likelihood of a VT very high (positive likelihood ratio 34.8). This criterion was successful in their own population of 163 selected patients and is awaiting prospective testing in a larger trial.
Vereckei aVR algorithm [5]


Griffith (Bundle Branch Block) algorithm
The Griffith algorithm [7]reverses the diagnostic strategy: unless simple rules for a positive diagnosis of supraventricular tachycardia are satisfied, ventricular tachycardia is diagnosed by default. The algorithm only looks at bundle brach block morphology. Supraventricular tachycardia is diagnoses when ECG findings match typical bundle branch block:
- LBBB: rS or QS wave in leads V1 and V2, delay to S wave nadir < 70 ms, and R wave and no Q wave in lead V6
- RBBB: rSR' wave in lead V1 and an RS wave in lead V6, with R wave height greater than S wave depth
Examples
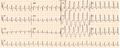
Wide complex tachycardia. No AV dissociation. RBBB. Resembles sinus rhythm from the same patient. Conclusion: SVT with RBBB
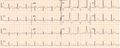
ECG from the same patient in sinus rhythm. The QRS complex is very similiar.
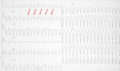
Wide complex tachycardia. LBBB configuration. Absence of RS in the chest leads. AV dissociation is present. Conclusion: VT
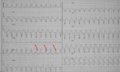
Wide complex tachycardia. LBBB configuration. Absence of RS in the chest leads. AV dissociation is present. Conclusion: VT


{kind=link}
Referenties
- Blomström-Lundqvist C, Scheinman MM, Aliot EM, Alpert JS, Calkins H, Camm AJ, Campbell WB, Haines DE, Kuck KH, Lerman BB, Miller DD, Shaeffer CW, Stevenson WG, Tomaselli GF, Antman EM, Smith SC Jr, Alpert JS, Faxon DP, Fuster V, Gibbons RJ, Gregoratos G, Hiratzka LF, Hunt SA, Jacobs AK, Russell RO Jr, Priori SG, Blanc JJ, Budaj A, Burgos EF, Cowie M, Deckers JW, Garcia MA, Klein WW, Lekakis J, Lindahl B, Mazzotta G, Morais JC, Oto A, Smiseth O, Trappe HJ, and European Society of Cardiology Committee, NASPE-Heart Rhythm Society. ACC/AHA/ESC guidelines for the management of patients with supraventricular arrhythmias--executive summary. a report of the American college of cardiology/American heart association task force on practice guidelines and the European society of cardiology committee for practice guidelines (writing committee to develop guidelines for the management of patients with supraventricular arrhythmias) developed in collaboration with NASPE-Heart Rhythm Society. J Am Coll Cardiol. 2003 Oct 15;42(8):1493-531. DOI:10.1016/j.jacc.2003.08.013 |
- Jastrzebski M, Kukla P, Czarnecka D, and Kawecka-Jaszcz K. Comparison of five electrocardiographic methods for differentiation of wide QRS-complex tachycardias. Europace. 2012 Aug;14(8):1165-71. DOI:10.1093/europace/eus015 |
- Brugada P, Brugada J, Mont L, Smeets J, and Andries EW. A new approach to the differential diagnosis of a regular tachycardia with a wide QRS complex. Circulation. 1991 May;83(5):1649-59. DOI:10.1161/01.cir.83.5.1649 |
- Pava LF, Perafán P, Badiel M, Arango JJ, Mont L, Morillo CA, and Brugada J. R-wave peak time at DII: a new criterion for differentiating between wide complex QRS tachycardias. Heart Rhythm. 2010 Jul;7(7):922-6. DOI:10.1016/j.hrthm.2010.03.001 |
- Vereckei A, Duray G, Szénási G, Altemose GT, and Miller JM. Application of a new algorithm in the differential diagnosis of wide QRS complex tachycardia. Eur Heart J. 2007 Mar;28(5):589-600. DOI:10.1093/eurheartj/ehl473 |
- Lau EW, Pathamanathan RK, Ng GA, Cooper J, Skehan JD, and Griffith MJ. The Bayesian approach improves the electrocardiographic diagnosis of broad complex tachycardia. Pacing Clin Electrophysiol. 2000 Oct;23(10 Pt 1):1519-26. DOI:10.1046/j.1460-9592.2000.01519.x |
- Griffith MJ, Garratt CJ, Mounsey P, and Camm AJ. Ventricular tachycardia as default diagnosis in broad complex tachycardia. Lancet. 1994 Feb 12;343(8894):386-8. DOI:10.1016/s0140-6736(94)91223-8 |